


I've spent several years helping medical students learn the best way to approach Step 1 studying, and the same pattern of feedback tends to come up repeatedly:
- “I knew the concept, but I overthink and talk myself out of the right answer.”
- “The real Step 1 felt more straightforward than the Qbank I used.”
- “I wish I spent more time on the fundamentals instead of tiny details.”
These frustrations share a common thread: the traditional Step 1 Qbank was built for a version of the exam that no longer exists.
They teach students to approach every question with suspicion, searching for obscure exceptions, and hunting for zebras. The modern Step 1, however, is designed to reward the student who can synthesize the entire clinical picture and apply high-yield foundational science.
Let me show you what changed, and how Bootcamp’s Step 1 Qbank was built for the updated exam.
What Changed on Step 1
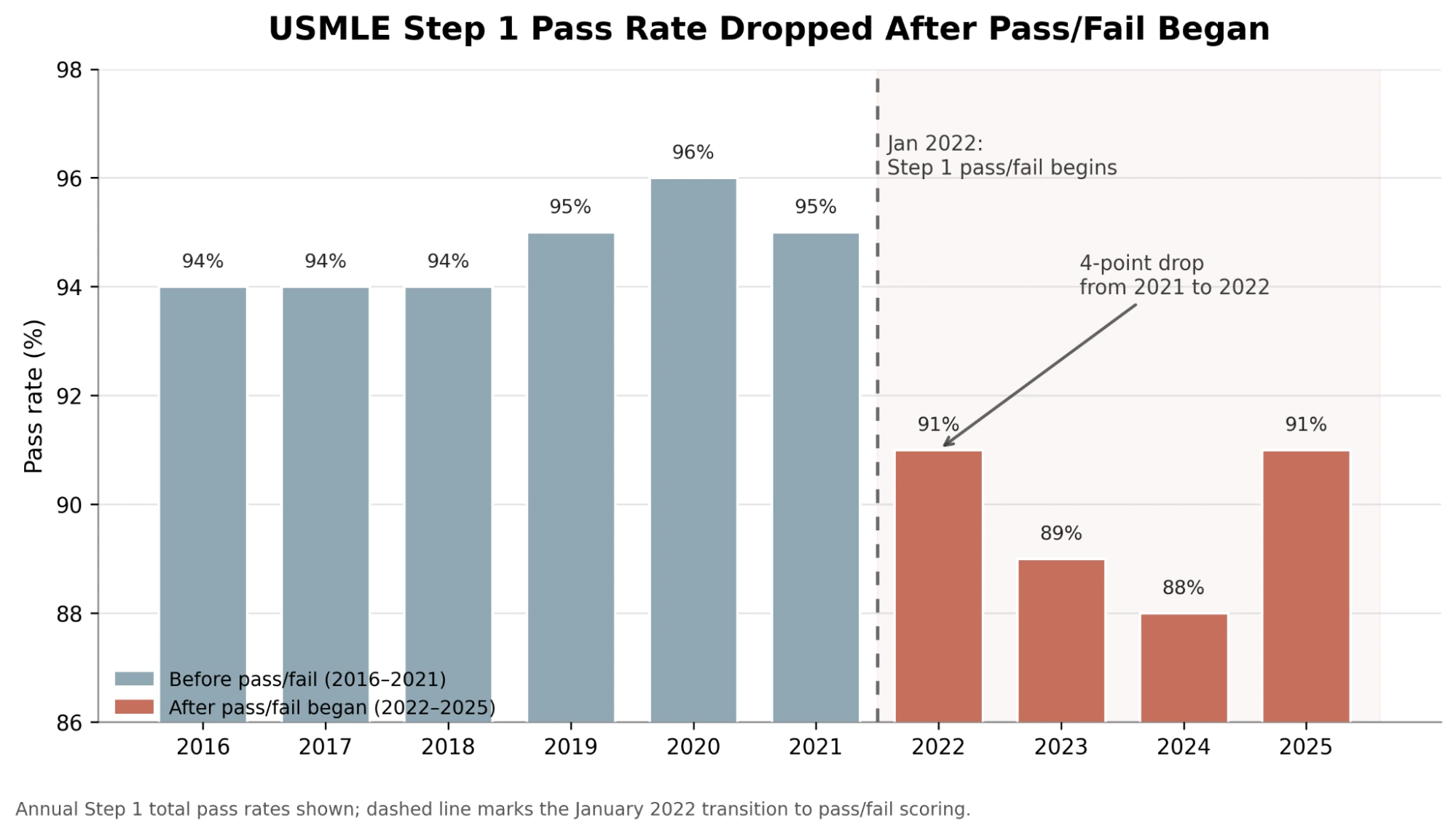
In January 2022, the USMLE transitioned Step 1 from a three-digit scoring system to a pass/fail outcome.[1] That did not make the exam easier. In fact, pass rates have declined since the transition.
This change fundamentally shifted the preparation paradigm, eliminating the necessity to memorize obscure, low-yield trivia to secure marginal point increases. The frantic search for every point between 240 and 260 was no longer a major factor.
So what does today’s exam reward? Roughly two-thirds is applying foundational science; a smaller fraction is diagnosis.[2] The majority of items are clinical vignettes presenting a patient’s demographics, medical history, physical examination findings, and diagnostic results.[3] The objective is to simulate the clinical reasoning process of a competent physician.
Furthermore, the National Board of Medical Examiners (NBME) item-writing guidelines explicitly instruct authors to avoid “tricky” phrasing or questions that reward test-taking strategies over genuine clinical knowledge.[4] The exam presents plausible clinical scenarios without attempting to deceive the examinee.
Two additional recent updates are highly relevant. First, communication and interpersonal skills now comprise 6% to 9% of the examination.[2] Second, as of June 2026, the USMLE significantly expanded its nutrition content across all three Step examinations, including the provision of specific feedback on nutrition in score reports.[5] Students tell us they study concepts in Bootcamp they’d never seen anywhere else and this is likely because legacy Qbanks that are retrofitted from a decade ago have a difficult time adjusting to the changes.
Many established resources contain thousands of questions (often exceeding 3,500 to 5,000 items) padded with low-yield questions and overly complex scenarios that were primarily relevant under the old three-digit scoring model. Consequently, these platforms train students defensively through divergent thinking, encouraging them to approach every clinical stem with suspicion and to anticipate rare anomalies (colloquially, “zebras”).
I believe this conditioned instinct is a primary reason students miss questions on the modern Step 1. They frequently overanalyze common clinical presentations, assume the question is trying to trick them, and subsequently disregard the correct answer. The failure is not in their knowledge base, but in a test-taking mindset calibrated for an exam that no longer exists.
What “Built for the Updated Step 1” Means
To address this discrepancy, the Bootcamp Qbank was developed specifically for the updated USMLE Step 1 framework. This alignment is achieved through four core principles:
Formatting Alignment: Question construction strictly revolves around the NBME methodology. The focus is on converging clinical findings rather than incorporating single esoteric details designed to mislead the examinee. Our Qbank prioritizes approximately 2,500 highly relevant questions, omitting artificial inflation with non-testable content.
Clinical Reasoning: Questions reward the comprehensive integration of the patient’s entire clinical picture rather than isolated pattern recognition of single terms in the last sentence of the question. The platform actively avoids setting traps that the actual exam does not employ.
Interface Accuracy: The testing interface accurately simulates the Prometric testing environment, including the most recent interface modifications implemented by the NBME.
Authoritative Review. Content is authored and rigorously reviewed by an in-house team of expert physicians, and iteratively refined based on extensive student feedback.
Let’s analyze a sample question from the Bootcamp Qbank:
Sample Question from the Bootcamp Qbank

Students accustomed to legacy question banks often develop a defensive test-taking strategy, reflexively anchoring on isolated keywords. For instance, a superficial reading might link “birds” directly to Chlamydia psittaci. Similarly, encountering the terms “humidifier” and “ventilation” might prematurely suggest Legionella pneumophila.
While these represent legitimate clinical associations—and pathogens like Histoplasma and Legionella are routinely tested concepts—relying solely on them often leads to answering a question that was not actually asked. This vignette reflects a converging methodology by including plausible single-exposure distractors, specifically rewarding the examinee who avoids premature diagnostic closure based on a single finding.
Let us approach this clinical vignette as a physician and synthesize the complete clinical picture. There are three distinct pathological processes occurring simultaneously, and the correct diagnosis must provide a unifying etiology for all three.
1. Atypical pneumonia: The patient is a young man presenting with a two-week history of a dry cough, low-grade fever, and diffuse bilateral crackles on exam.
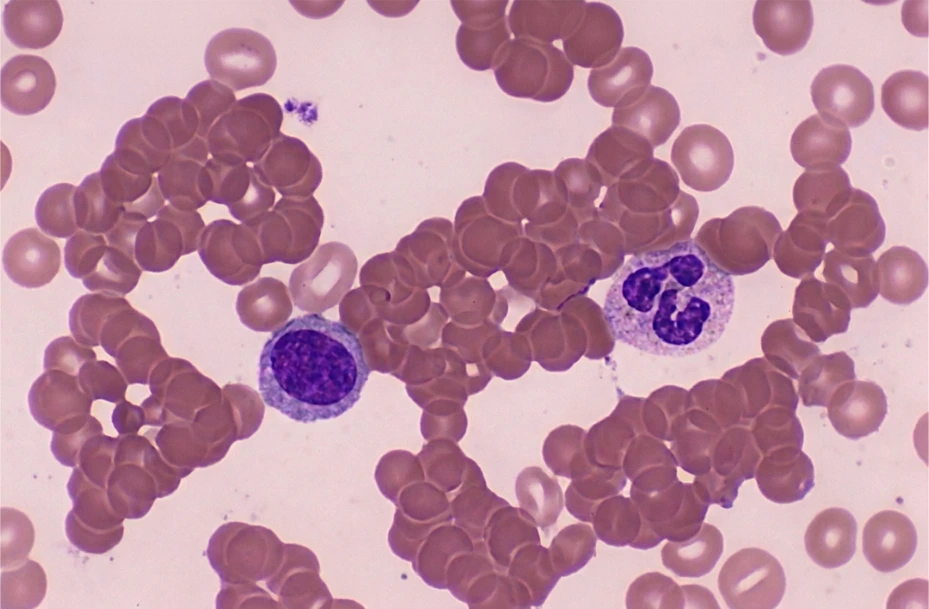
2. Hemolytic anemia: The hemoglobin is 9.8 g/dL with an appropriately elevated reticulocyte count, indicating a robust bone marrow response. The patient’s tachycardia and sudden fatigue are likely clinical manifestations of acute anemia. The bilirubin profile provides further diagnostic insight: a total bilirubin of 4.2 mg/dL with a direct fraction of only 0.4 mg/dL indicates predominant indirect (unconjugated) hyperbilirubinemia. This finding is consistent with hemolysis and corresponds clinically to the observed scleral icterus. The diagnostic hallmark is a direct antiglobulin test (DAT or Coombs test) that is positive for C3d and negative for IgG, accompanied by erythrocyte agglutination on peripheral blood smear.[7] This pattern indicates the presence of cold agglutinins, which are IgM autoantibodies that cross-react with the I antigen on erythrocytes. [6] In the cooler peripheral circulation, IgM binds to erythrocytes and fixes complement (resulting in a C3d-positive DAT), culminating primarily in extravascular hemolysis. The patient’s acrocyanosis clinically corroborates this mechanism.
3. Target lesions: Erythematous papules with a dusky center and a pale ring, on the palms. This is textbook erythema multiforme.
The next step is to identify the convergence of these key findings. What single organism accounts for an atypical pneumonia, IgM cold-agglutinin hemolysis, and erythema multiforme in a young man living in crowded conditions whose illness is resistant to amoxicillin? Mycoplasma pneumoniae
The mechanism is elegant and testable. Mycoplasma adheres to the I antigen located on the respiratory epithelium. Because the same I antigen is expressed on erythrocytes, the subsequent humoral response generates cross-reactive anti-I IgM antibodies (cold agglutinins). (Note: Mycoplasma is associated with anti-I antibodies, whereas Epstein-Barr virus [EBV], the causative agent of infectious mononucleosis, is associated with anti-i antibodies.)[6]
Mycoplasma is also a well-established trigger for erythema multiforme.[8] Furthermore, the lack of clinical improvement with amoxicillin is diagnostically significant: because Mycoplasma lacks a peptidoglycan cell wall, it is inherently resistant to beta-lactam antibiotics. Appropriate pharmacotherapy includes a macrolide, doxycycline, or a respiratory fluoroquinolone.[9]
Evaluating the incorrect explanations are just as critical for learning as reviewing the correct ones. Looking back at two of the more classically tested distractors:
Legionella [Choice C]: The patient’s normal serum sodium concentration (141 mEq/L) and the absence of neurological symptoms (eg., headache) or gastrointestinal symptoms decrease the clinical likelihood of Legionella pneumophila infection, which classically presents with hyponatremia and gastrointestinal manifestations. [10]
Chlamydia [Choice D]: While Chlamydia species, including Chlamydia pneumoniae, are established etiologies of atypical pneumonia, and Chlamydia psittaci is specifically associated with avian exposure, [11] neither of these pathogens is characteristically associated with cold agglutinin-mediated hemolysis, acute anemia, or erythema multiforme.
The preceding breakdown showcases the anatomy of a single question: an authentic clinical presentation, NBME-aligned clinical reasoning, Prometric-simulated interface integration, and high yield distractors.
Every Explanation is a Masterclass in Medicine
The real value of a question comes after a student misses it. That is why Bootcamp explanations are built differently to not just justify the answer, but teach the medicine behind the answer.
Each explanation is designed to help students understand the concept at the level Step 1 actually tests it: clinically, mechanistically, and visually. When an explanation references a concept that students commonly struggle with, we connect it back to the relevant Bootcamp video lesson, visual, or high-yield table. The student is not left to patch together disconnected resources. The question, explanation, video, and review material are designed to reinforce the same mental model.
That philosophy extends beyond the written explanation itself.
- Visual Learning: Our explanations incorporate labeled illustrations, histopathology, radiographic images, clinical photographs, flowcharts, and summary tables so students can build lasting visual associations alongside conceptual understanding.
- Comprehensive Clinical Reasoning: Every explanation walks through the thought process, not just the answer. Students learn how to synthesize the vignette, identify the pivotal clues, eliminate attractive distractors, and connect the underlying physiology, pathology, microbiology, and pharmacology into a coherent framework. The goal is not simply to answer one question correctly, but to answer the next five questions on the same concept correctly.
- Unlimited AI Tutoring: Every question includes access to Ask Bootcamp AI, allowing students to ask unlimited follow-up questions directly within our Qbank interface, without the usage constraints found in other legacy Qbanks.
- Seamless Anki Integration: For long-term knowledge retention, our platform integrates AnKing card IDs into the Qbank. You can just simply click “Get Anki Cards”, and this drops the matching AnKing cards into your deck (with the latest AnKing on AnkiHub).[12]
- Linked Video Lessons: Questions link directly to high-yield videos for any concepts that you are having a hard time understanding.
In other words, every missed question becomes an opportunity to revisit the underlying concept from multiple angles – text, visuals, video, flashcards, and interactive tutoring – all within a single learning environment.
Then We Applied This Methodology Across More Than 2,500 Questions
Every one of our approximately 2,500 questions was designed around the same principles: authentic NBME-style clinical reasoning, modern Step 1 content, comprehensive explanations, and integrated learning tools. We deliberately prioritized quality over quantity, focusing on the questions students are actually likely to benefit from rather than inflating the database with increasingly obscure edge cases.
Because the USMLE continues to evolve, our Qbank does too. New content areas, changing exam emphasis, and student feedback continually shape revisions to existing questions and the development of new ones. Rather than treating the Qbank as a static product, we view it as an evolving educational resource built for the current version of Step 1.
Beyond the questions themselves, we've added tools that help students study more efficiently throughout dedicated:
- Performance analytics that identify strengths and weaknesses across disciplines and organ systems.
- Pass prediction metrics that provide an objective assessment of readiness.
- Study schedule optimization to help students prioritize what to review next.
See the Difference for Yourself
Ultimately, the easiest way to understand what makes Bootcamp different is to use it.
The free trial includes 3 days of full access to every feature, no credit card required.
Try a question block, read an explanation, watch the linked video, ask Bootcamp AI a few questions, and open the matching AnKing cards. You will quickly see how the pieces fit together into a single learning platform rather than a disconnected collection of questions.
And if you decide Bootcamp is right for you, every 1- and 2-year membership is backed by our Pass Guarantee, reflecting the confidence we have in the platform we've built.
Step 1 has changed. The way students prepare for it should change too.
If you’re preparing for Step 1, start your free trial and experience the Qbank built for the updated exam.
References
Each source below was located by one agent and then independently re-opened and checked by a separate reviewer agent that confirmed the source actually states the claim. Titles are clickable.
[1] USMLE — “Step 1 pass/fail score reporting implementation date”. (Announced Feb 12, 2020; pass/fail-only reporting for exams taken on or after Jan 26, 2022.)
[2] USMLE — “Step 1 Content Outline and Specifications” (Physician Tasks/Competencies). (Applying Foundational Science Concepts 60–70%; Diagnosis 20–25%; Communication & Interpersonal Skills 6–9% of items. Supports the “two-thirds foundational science,” “smaller fraction diagnosis,” and “6% to 9% communication” statements.)
[3] USMLE — “Step 1 Test Question Formats”. (Each item is built around a single patient-centered clinical vignette.)
[4] National Board of Medical Examiners — Constructing Written Test Questions for the Basic and Clinical Sciences (Paniagua MA, Swygert KA, eds.). (Item stems should “not be ‘tricky’ or overly complex” and should avoid “testwiseness” flaws that reward test-taking skill over knowledge. Authentic NBME manual, hosted on a university faculty-development mirror.)
[5] USMLE — “Enhancements to Nutrition Content on USMLE Step Exams Coming in June 2026”. (Nutrition content enhanced across all three Step exams; nutrition performance feedback added to examinee and medical-school score reports.)
[6] Berentsen S. New Insights in the Pathogenesis and Therapy of Cold Agglutinin-Mediated Autoimmune Hemolytic Anemia. Front Immunol. 2020. (Cold agglutinins are anti-I specific IgM in M. pneumoniae, and anti-i in EBV/CMV infection. PMID 32318071.)
[7] Gabbard AP, Booth GS. Cold Agglutinin Disease. Clin Hematol Int. 2020. (Nearly all cold agglutinins are C3d DAT-positive; hemolysis is complement-mediated and predominantly extravascular via Kupffer cells. PMID 34595449.)
[8] Trayes KP, et al. Erythema Multiforme. StatPearls, NCBI Bookshelf. 2023. (M. pneumoniae is a common cause of erythema multiforme, particularly in children.)
[9] Pereyre S, Goret J, Bébéar C. Mycoplasma pneumoniae: Current Knowledge on Macrolide Resistance and Treatment. Front Microbiol. 2016. (Lacks a cell wall, so it is resistant to beta-lactams; intrinsically susceptible to macrolides, tetracyclines, and fluoroquinolones. PMID 27446015.)
[10] Darby J, Buising K. Could it be Legionella? Aust Fam Physician. 2008. (Clinical clues include gastrointestinal symptoms/diarrhoea, neurological symptoms, hyponatraemia, and hepatic dysfunction. PMID 19002299.)
[11] Rybarczyk J, et al. Human psittacosis: a review with emphasis on surveillance in Belgium. Acta Clin Belg. 2019. (Chlamydia psittaci causes psittacosis, mainly in people in contact with birds. PMID 30882289.)
[12] Price DW, et al. The Effect of Spaced Repetition on Learning and Knowledge Transfer in a Large Cohort of Practicing Physicians. Acad Med. 2024. (Spaced repetition — the mechanism Anki implements — is superior to repeated study for learning and long-term retention. PMID 39250798.)



Get everything you need in one place. Start studying today for free.












